A BURDEN IN MY HEART
I just returned from Yangon, Myanmar, a couple of weeks ago. That was my third trip this year, to conduct a series of training, for teachers, parents and other professionals (Physiotherapists, Principals, Psychologists, etc). It has been an awesome journey working with professionals who are so eager to learn, in Myanmar, where they have very limited Speech Therapy services. (There is only one practicing Speech Therapist in Yangon, Myanmar at the time of this writing.)
Between my previous trip in May and my latest trip in August, I came to know that TalkToolsⓇ and ARK Therapeutic tools are now available in Myanmar. On one hand, I am very happy and excited about the availability. On the other hand, I am worried.
There are two main considerations:
Using OPT as an Only Approach to Speech Delay
When I first started out as a Speech Therapist in 2008, Oral Placement Therapy (OPT; then known as Oral Motor Therapy) was a big thing in Singapore. Many parents bought the therapy tools in bulk. These tools gave them hope for their children who are not speaking yet. It was something concrete for them to hold on to. OPT goals are much more concrete and measurable, as compared to language goals and/or pre-verbal skills goals.
I also heard of speech therapists who saw it as a business opportunity, saying that they specialised in OPT. They prescribed tonnes of exercises. However, when the results of having speech did not follow, the therapists blamed parents for their lack of diligence in following the exercise programme rigidly. Many parents were let down and also felt ashamed.
I am not saying that OPT is not good. On the contrary, I do quite a bit of OPT and use the tools in my sessions. I have seen wonderful results. However, we must use OPT and its tools with caution. It must never be used as an ONLY approach for delayed speech; it should always be used in adjunct to other therapy approaches.
Firstly, there is no strong evidence to show that the use of OPT will produce speech.
Secondly, there are many reasons why a child is not having speech yet. It could be due to motor planning difficulties. It could be due to muscles weakness. It could be due to poor pre-verbal and language skills. It could be due to cognitive delay. Most often, the lack of speech is due to multiple reasons. As such, using OPT alone is not going to show results.
I feel burdened that the parents of Myanmar might be misled into thinking that OPT is THE answer to their children who are not talking yet.
Prescription of Home Programme by Non-Speech Therapist Professionals
I had my OPT training in April 2010, after using OPT for nearly 2 years. (Before my OPT training, I had used it under the supervision of my Speech Therapy seniors.) After the training, I felt more competent in using the tools and prescribing a home programme; however, I was still not 100% sure that what I had prescribed would work because OPT is not evidence-based. Even with my Speech Therapy degree, clinical experience of 2 years and full-fledged OPT workshops, I never quite grasp the principles of OPT. Most importantly, I had always looked at a child neck-up, until I obtained my Neuro-Developmental Treatment (NDT) certification in August 2010. NDT taught me how to look at a child from the toes to the head - problems with the jaw/lips/tongue are never just problems with the jaw/lips/tongue.
With my Speech Therapy degree and subsequent professional training/certifications, as well as my clinical experience of nearly 10 years, I could say I am now confident in prescribing an OPT Programme. I would prescribe the tools based on the underlying principles of motor development, never just following the OPT manuals rigidly.
My burden for Myanmar, where there is only one practicing Speech Therapist, is that non-Speech Therapist professionals are prescribing OPT programmes. They could be ABA therapists, psychologists or special education teachers, who were said to have attended OPT workshops, either physically or online. OPT workshops may provide enough knowledge to carry out an OPT programme, but definitely not enough to start prescribing OPT programmes. Some of the prescribed programmes are extensive, but when I did a review, caregivers were not using the correct techniques and the children were practicing the exercises wrongly. For example, when a child works on his jaw strength using the chewy tubes, the jaw is not aligned; this is detrimental as the compensatory patterns of misaligned chewing were reinforced. Not only will the child not improve, it will result in malfunctioned movement patterns. In addition, many times when a child presents with a weak jaw, the problem stems from a weak core. Physiotherapy and/or Occupational Therapy will be required. Just working on the jaw alone will not be effective.
Having said all that, I have spoken to the distributor of the tools and shared my burden. She shared that she has a child with special needs and assured that she will remind fellow parents that OPT is not THE solution to a child's speech problems, and that consultation with a Speech Therapist is highly recommended.
I pray for the Myanmar children with special needs and their families.

Between my previous trip in May and my latest trip in August, I came to know that TalkToolsⓇ and ARK Therapeutic tools are now available in Myanmar. On one hand, I am very happy and excited about the availability. On the other hand, I am worried.
There are two main considerations:
Using OPT as an Only Approach to Speech Delay
When I first started out as a Speech Therapist in 2008, Oral Placement Therapy (OPT; then known as Oral Motor Therapy) was a big thing in Singapore. Many parents bought the therapy tools in bulk. These tools gave them hope for their children who are not speaking yet. It was something concrete for them to hold on to. OPT goals are much more concrete and measurable, as compared to language goals and/or pre-verbal skills goals.
I also heard of speech therapists who saw it as a business opportunity, saying that they specialised in OPT. They prescribed tonnes of exercises. However, when the results of having speech did not follow, the therapists blamed parents for their lack of diligence in following the exercise programme rigidly. Many parents were let down and also felt ashamed.
I am not saying that OPT is not good. On the contrary, I do quite a bit of OPT and use the tools in my sessions. I have seen wonderful results. However, we must use OPT and its tools with caution. It must never be used as an ONLY approach for delayed speech; it should always be used in adjunct to other therapy approaches.
Firstly, there is no strong evidence to show that the use of OPT will produce speech.
Secondly, there are many reasons why a child is not having speech yet. It could be due to motor planning difficulties. It could be due to muscles weakness. It could be due to poor pre-verbal and language skills. It could be due to cognitive delay. Most often, the lack of speech is due to multiple reasons. As such, using OPT alone is not going to show results.
I feel burdened that the parents of Myanmar might be misled into thinking that OPT is THE answer to their children who are not talking yet.
Prescription of Home Programme by Non-Speech Therapist Professionals
I had my OPT training in April 2010, after using OPT for nearly 2 years. (Before my OPT training, I had used it under the supervision of my Speech Therapy seniors.) After the training, I felt more competent in using the tools and prescribing a home programme; however, I was still not 100% sure that what I had prescribed would work because OPT is not evidence-based. Even with my Speech Therapy degree, clinical experience of 2 years and full-fledged OPT workshops, I never quite grasp the principles of OPT. Most importantly, I had always looked at a child neck-up, until I obtained my Neuro-Developmental Treatment (NDT) certification in August 2010. NDT taught me how to look at a child from the toes to the head - problems with the jaw/lips/tongue are never just problems with the jaw/lips/tongue.
With my Speech Therapy degree and subsequent professional training/certifications, as well as my clinical experience of nearly 10 years, I could say I am now confident in prescribing an OPT Programme. I would prescribe the tools based on the underlying principles of motor development, never just following the OPT manuals rigidly.
My burden for Myanmar, where there is only one practicing Speech Therapist, is that non-Speech Therapist professionals are prescribing OPT programmes. They could be ABA therapists, psychologists or special education teachers, who were said to have attended OPT workshops, either physically or online. OPT workshops may provide enough knowledge to carry out an OPT programme, but definitely not enough to start prescribing OPT programmes. Some of the prescribed programmes are extensive, but when I did a review, caregivers were not using the correct techniques and the children were practicing the exercises wrongly. For example, when a child works on his jaw strength using the chewy tubes, the jaw is not aligned; this is detrimental as the compensatory patterns of misaligned chewing were reinforced. Not only will the child not improve, it will result in malfunctioned movement patterns. In addition, many times when a child presents with a weak jaw, the problem stems from a weak core. Physiotherapy and/or Occupational Therapy will be required. Just working on the jaw alone will not be effective.
Having said all that, I have spoken to the distributor of the tools and shared my burden. She shared that she has a child with special needs and assured that she will remind fellow parents that OPT is not THE solution to a child's speech problems, and that consultation with a Speech Therapist is highly recommended.
I pray for the Myanmar children with special needs and their families.

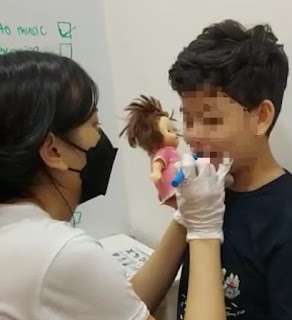
Reviewing an OPT home programme in Myanmar,
ensuring that the teachers use the correct techniques and know what to look out for.


Comments
Post a Comment